


ENTER THE SACRED BACKYARD
SACRED SOUL FAMILY

Dodee is a Certified Holistic Health Practitioner, certified in Dr. Klinghardt's Autonomic Response Testing, and is an educator of the Living Biofield as an integral part of health, with nearly two decades of experience in detox strategies, holistic healing, and long-standing chronic illness. Dodhisattva.com, est. 2009
Tinnitus and menopause occurring around the same time are often overlooked.
That ringing, buzzing, or humming in your ears that seemed to appear out of nowhere during perimenopause or menopause is something a significant number of women experience.
Some studies suggest that up to one-third of women going through this transition notice new or worsening tinnitus, and menopause is happening at the same time.
Yet most are told there is nothing to be done.
This article takes a different look at the biology of what is actually happening.
When you understand the connection among your hormones, your stress response, and your auditory system, the pieces start to fit together for tinnitus and menopause in a way that points toward real, natural support strategies rather than a shrug and a prescription.
We are going to cover the estrogen-tinnitus connection, the often-overlooked role of cortisol in making tinnitus worse, the nutrients your auditory neurons may be depleted in, and what emerging research and integrative practitioners are finding may support the auditory system naturally.
Tinnitus is not a disease. It is a symptom, a signal that something in the auditory pathway is not working the way it should.
The ringing, buzzing, or hissing is not coming from outside.
It is generated internally, most often by hyperactive auditory neurons in the brain that fire in the absence of real sound input.
For most of your reproductive life, estrogen quietly supported your auditory system in ways you never had to think about.
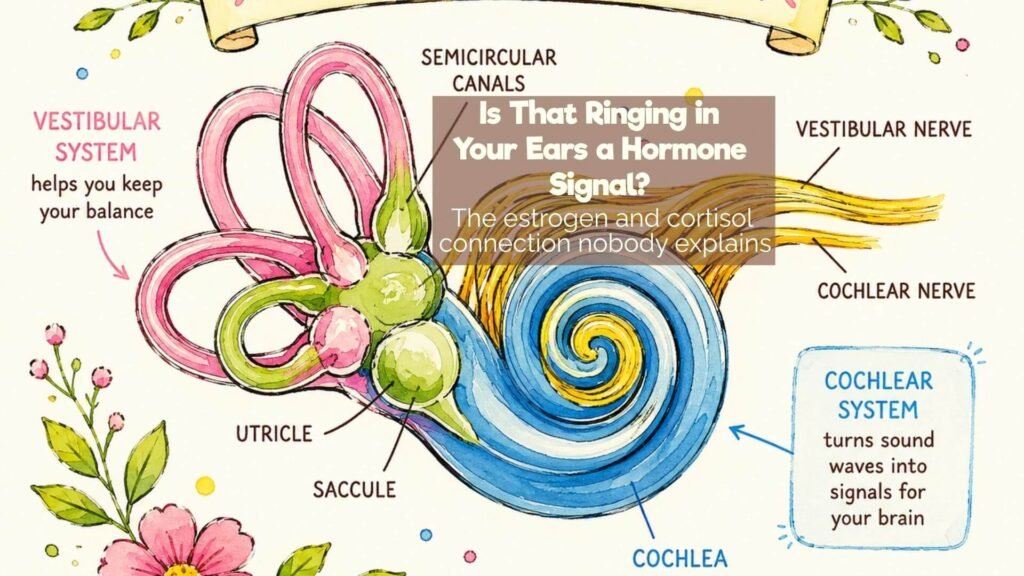
Estrogen receptors are found throughout the cochlea, which is the spiral structure of the inner ear responsible for converting sound vibrations into nerve signals.
Estrogen supports healthy blood flow to the cochlea, protects the delicate hair cells that are responsible for sound transduction, and helps regulate the neurotransmitters that keep auditory processing stable and filtered.
When estrogen declines during perimenopause and menopause, these protective effects weaken.
Blood flow to the cochlea can decrease. Hair cells become more vulnerable. The brain’s ability to filter out background noise and phantom signals starts to slip.
This is why tinnitus and menopause so often arrive together. It is hormonal biology, not coincidence.
Research confirms this connection. Studies have found that women with tinnitus tend to have lower estrogen levels compared to those without it, suggesting estrogen plays a protective role in auditory function.
When those levels drop, the system loses some of its natural buffering.

Here is where the tinnitus and menopause picture gets more layered.
As ovarian hormone production declines, the adrenal glands are meant to pick up some of the slack.
But if the adrenals are already working hard from years of stress, illness, or chronic demands, they often cannot make this transition smoothly.
The result is elevated cortisol, the body’s primary stress hormone, running higher than it should.
Cortisol and tinnitus have a well-documented relationship.
Research published in Frontiers in Systems Neuroscience showed that chronic stress activates the hypothalamic-pituitary-adrenal axis in ways that directly alter neural excitability in the auditory cortex.
Functional MRI scans of people with tinnitus show hyperactivity in the auditory cortex alongside increased activity in the amygdala and hippocampus, the brain regions involved in fear, memory, and stress processing.
In plain terms, elevated cortisol turns up the volume on the auditory system’s threat monitoring.
What might have been a barely noticeable background hiss becomes an intrusive, loud signal.
The brain, primed by cortisol to scan for danger, starts treating the phantom sound as something worth paying attention to.
This is why tinnitus almost universally worsens during periods of acute stress and why managing the stress response is not just a soft lifestyle recommendation but a genuine physiological target.
One study measuring serum cortisol in tinnitus patients found that cortisol levels could be used as an effective indicator of stress status in people with tinnitus.
The relationship is bidirectional too.
Tinnitus itself becomes a stressor, elevating cortisol further, which then amplifies the tinnitus.
It is a feedback loop that is hard to escape without addressing the cortisol piece directly.
Additionally, research has found that individuals with tinnitus show a deficit in GABA, the brain’s primary inhibitory neurotransmitter, specifically in the right side of the auditory cortex.
Cortisol chronically depletes GABA over time. Less GABA means less inhibition of auditory neuron firing. Less inhibition means more phantom sound.

Soy free. Silica free. Practitioner grade. Phosphatidylserine for cortisol regulation, brain membrane support, and auditory neuron health.
Phosphatidylserine is a phospholipid that sits within the membranes of every cell in your body, but it is most highly concentrated in brain cell membranes, particularly in the hippocampus and auditory cortex.
It has an important role in how neurons fire, how neurotransmitters are released, and how the brain’s stress response system knows when to stand down.
The connection to tinnitus and menopause runs through several pathways simultaneously.
First, phosphatidylserine supports the membrane stability of auditory neurons.
When neuronal membranes are depleted or compromised, those neurons become hyperexcitable, which is precisely the state that generates phantom sounds.
Restoring membrane integrity may help bring that hyperexcitability back toward a more regulated baseline.
Second, phosphatidylserine is one of the more well-researched natural tools for modulating the HPA axis and lowering cortisol.
Multiple studies have shown that supplementation can blunt the cortisol stress response by supporting hippocampal function, which is the brain region responsible for signaling the adrenal glands to reduce cortisol output.
Given the cortisol-tinnitus relationship described above, this is not a small thing.
Third, estrogen normally helps maintain phosphatidylserine levels in brain cell membranes.
When estrogen declines in menopause, brain phosphatidylserine levels tend to fall with it.
This is one of the reasons menopausal women may respond so noticeably to phosphatidylserine supplementation.
Research suggests that 300 mg per day, spaced throughout the day, is needed at least in the beginning.
The brain has been running on depleted reserves and recognizes what it has been missing.
Fourth, phosphatidylserine is a component of myelin, the protective sheath around nerve fibers including the auditory nerve, which is one of the most heavily myelinated structures in the body.
Myelin integrity affects the quality and clarity of signal transmission from the cochlea to the brain. Degraded myelin means degraded signal, which the brain may interpret as distortion or phantom noise.
A product called MemoVigor2, which contains phosphatidylserine alongside other phospholipids and nutrients, has been specifically studied and marketed in the context of tinnitus support, providing some clinical acknowledgment that this phospholipid family has relevance to auditory neuron health.
Users in tinnitus communities have shared experiences of reduced tinnitus intensity while supplementing with phosphatidylserine, with some attributing the change specifically to its cortisol-lowering effects.
It is worth noting that research in this area is still emerging.
Phosphatidylserine is not a cure for tinnitus, and individual responses vary.
What the science does suggest is that supporting neuronal membrane health and modulating the cortisol stress response is a physiologically sound approach to creating an internal environment where the auditory system can function with less interference.
Beyond phosphatidylserine, several other nutrients and practices show up consistently in both research and integrative clinical settings for tinnitus support.
Magnesium is one of the most studied.
It plays a role in protecting the delicate structures of the inner ear and supports blood flow to the cochlea.
Research has found that low magnesium levels are associated with increased susceptibility to noise-induced hearing changes and that supplementation may help reduce tinnitus intensity in some individuals.
You might enjoy my magnesium bath recipe here.
Magnesium also supports GABA production, addressing the neurotransmitter deficit described above.
Zinc has a documented connection to tinnitus risk. A 2024 study found that low zinc levels increased tinnitus risk by 44 percent.
Zinc is concentrated in the cochlea and plays a role in protecting auditory hair cells.
Vitamin B12 deficiency has been associated with tinnitus, particularly in older women.
Higher intake has been linked to meaningful symptom reduction in some research.
Getting levels checked is worth considering.
Blood flow to the cochlea matters significantly because it has no backup blood supply.
Anything that supports healthy microcirculation, including regular movement, staying well hydrated, and reducing inflammatory foods, supports the cochlea’s ability to function well.
Stress regulation practices are not soft add-ons.
One of the most important things to do is to start calming yourself down when you recognize the fight-or-flight response.
Do what you can to make it a new habit.
For example, are you racing to eat or racing to get up in the morning to brush your teeth?
Taking a deep breath with a very slow exhale and moving a bit more mindfully is a free way to start lowering that cortisol response.
Mindfulness, breathwork, and yoga have shown measurable effects on tinnitus perception in clinical studies.
Some of my guided meditations may help here.
When the nervous system shifts out of chronic sympathetic activation, the auditory cortex quiets with it.
This is the same mechanism phosphatidylserine addresses biochemically, just through a different route.
Progesterone is worth a mention, specifically for menopausal women.
Progesterone is neuroprotective and anti-inflammatory.
As it declines in perimenopause and menopause, the brain and nervous system lose some of their natural cushioning.
Bioidentical progesterone support is something worth discussing with a knowledgeable integrative practitioner in the context of overall hormonal balance and its downstream effects on neurological symptoms, including tinnitus.
This is one of the most searched questions around tinnitus and menopause, and the honest answer is that it depends.
For some women, tinnitus does quiet as hormones stabilize post-menopause.
For others, it persists or becomes chronic if the underlying drivers, particularly cortisol dysregulation and nutritional depletion, are not addressed.
A UCI Health otolaryngologist described it this way: estrogen helps regulate blood flow in the inner ear, supports the hair cells that convert sound into signals, and stabilizes the brain networks that filter out background noise.
When estrogen levels swing or drop, these systems can become destabilized, leading to heightened auditory sensitivity.
The good news is that when hormones stabilize post-menopause, some women do find the ringing fades or becomes easier to live with.
What appears to make the biggest difference is how well the cortisol piece is managed through the transition.
Women who support their adrenal function, maintain stable blood sugar, address nutritional depletions, and work with their nervous system during perimenopause tend to report better outcomes on the other side.
Tinnitus and menopause share a common hormonal and neurological root.
Declining estrogen removes a layer of protection from the auditory system.
Rising cortisol turns up the brain’s internal volume dial.
Nutritional depletions in phosphatidylserine, magnesium, zinc, and B12 leave auditory neurons working with less than they need.
The phantom sounds that result are real and they are connected to real biological shifts that can be meaningfully supported.
Supporting the auditory system naturally during menopause is not about chasing a cure.
It is about restoring the conditions under which your nervous system and auditory pathways can function with greater stability.
That means working with hormonal balance, managing the cortisol response, rebuilding neuronal membrane integrity, and ensuring the raw nutritional materials your ears and brain need are actually available.
If you are experiencing tinnitus during perimenopause or menopause, you are not alone and you are not without options.
Working with an integrative practitioner who understands both hormonal health and neurological support can help you build a protocol that addresses the real drivers rather than just masking the symptom.
This article is for informational and educational purposes only and does not constitute medical advice. Nothing here is intended to diagnose, treat, cure, or prevent any disease or health condition. Individual results vary. Always consult a qualified healthcare practitioner before beginning any new supplement or health protocol.

POPULAR POSTS
MEDITATIONS
It’s FREE! And I know you’re going to love it.